Alcohol Use Disorder: A Crisis Demanding New Solutions
The Scale of the Problem
48M+
Europeans affected by Alcohol Use Disorder — over 10% of the adult population.
>60%
Relapse rate even with the best available pharmacological and psychosocial treatments.
2.6%
Of EU GDP lost to alcohol-related harm — healthcare costs, productivity losses, and social damage.
The Relapse Mechanism
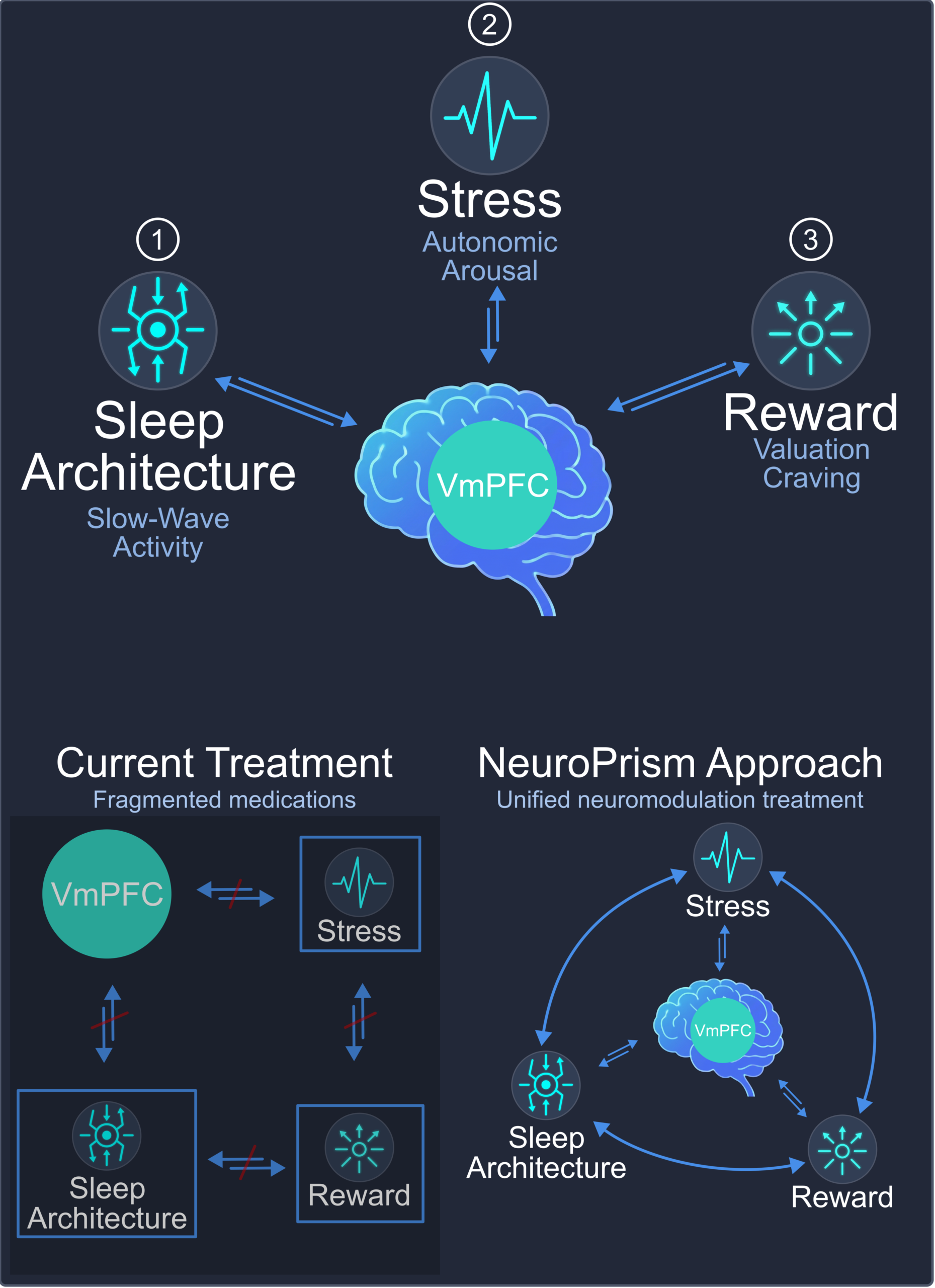
Converging neuroscience evidence points to a shared mechanism driving AUD relapse — centered on the ventromedial prefrontal cortex (vmPFC).
The vmPFC sits at the intersection of three critical systems disrupted in AUD:
Sleep architecture: The vmPFC regulates slow-wave activity and sleep stability. Alcohol disrupts these processes, and the resulting sleep disturbances persist well into abstinence — creating a physiological vulnerability to relapse.
Stress and arousal regulation: Dysregulated vmPFC control over autonomic arousal drives the stress hyperactivity that characterizes early recovery. Poor sleep amplifies this effect, creating a vicious cycle.
Reward valuation and craving: The vmPFC assigns value to rewards and exerts top-down control over craving-related striatal activity. When vmPFC function is impaired, craving signals go unchecked — leading to relapse.
This creates a mechanistic pathway: sleep disruption → stress hyperarousal → impaired vmPFC regulation → craving and relapse.
Why Current Treatments Fall Short
Pharmacotherapy
Naltrexone and acamprosate reduce craving but are limited by significant side effects — including sleep disruption and mood disturbances — that ironically worsen the very symptoms driving relapse. Compliance remains a major challenge: many patients discontinue medication within weeks.
Current pharmacotherapy and psychosocial treatments address craving and sleep as separate problems, missing the shared neural substrate (vmPFC circuitry) that connects them.
Existing Neuromodulation
Transcranial magnetic stimulation (TMS) can modulate brain circuits non-invasively, but it cannot reach deep targets like the vmPFC — its effects are limited to the cortical surface. Transcranial direct current stimulation (tDCS) reaches deeper but lacks focality, spreading current diffusely across the brain.
Neither technology is portable or suitable for home use. Both require clinic visits that limit scalability and patient adherence, and neither has demonstrated consistent efficacy in AUD.